2010年10月30日 星期六
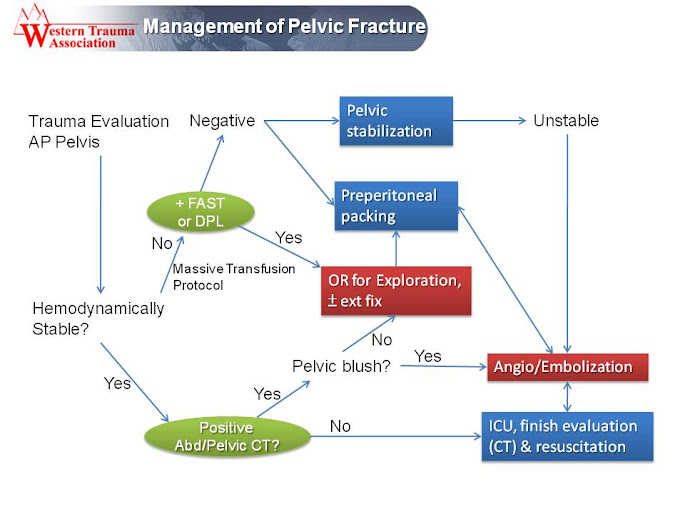
Management of Pelvic Fracture with Hemodynamic Instability
Western Trauma Association Critical Decisions in Trauma:
Management of Pelvic Fracture with Hemodynamic Instability
J. Trauma. Volume 65 (5), November 2008, pp 1007-1011
2010年10月26日 星期二
Adult Stroke
Stroke (2010 Guideline for CPR & ECC)
Adult Strok
View more presentations 按畫面中央的 Click to Play 後,再按下方的 ►即可播放
獨家製作,版權沒有,歡迎 下載2010 AHA Guidelines for CPR and ECC
Circulation. 2010;122:S818-S828
The “D's of Stroke Care”
- Detection: Rapid recognition of stroke symptoms
- Dispatch: Early activation and dispatch of EMS system by calling 911
- Delivery: Rapid EMS identification, management, and transport
- Door: Appropriate triage to stroke center
- Data: Rapid triage, evaluation, and management within the ED
- Decision: Stroke expertise and therapy selection
- Drug: Fibrinolytic therapy, intra-arterial strategies
- Disposition: Rapid admission to stroke unit or ICU
- Time is Brain
- Minimize acute brain injury and maximize patient recovery
- Stroke Chain of Survival
- Cincinnati Prehospital Stroke Scale (CPSS)
Sensitivity: 59%; Specificity: 89%
- Los Angeles Prehospital Stroke Screen (LAPSS)
In-Hospital CareSensitivity: 93%; Specificity: 97%
- Protocols should be used in the ED to minimize delay to definitive diagnosis and therapy.
- ED personnel should assess the patient with suspected stroke within 10 minutes of arrival in the ED.
- The EP should perform a neurologic screening assessment, order emergent CT, and activate the stroke team.
- Patient eligible for acute reperfusion therapy except that BP >185/110 mmHg
- Labetalol 10 to 20 mg IV over 1 to 2 minutes, may repeat ×1
- If BP does not below 185/110 mmHg, do not administer rtPA
- If SBP 180–230 mmHg or DBP 105–120 mmHg
- Labetalol 10 mg IV followed by continuous IV infusion 2–8 mg/min
- If BP not controlled or diastolic BP >140 mmHg, consider sodium nitroprusside
- Consider lowering BP in acute ischemic stroke if BP >220/120 mmHg
- A reasonable target is to lower BP by 15% to 25% within the first day
Inclusion and Exclusion Characteristics of Patients with Ischemic Stroke Who Could Be Treated with rtPA within 3 Hours from Symptom Onset
Inclusion Criteria
- Diagnosis of ischemic stroke causing measurable neurologic deficit
- Onset of symptoms <3 hours before beginning treatment
- Age >18 years
- Head trauma or prior stroke in previous 3 months
- Symptoms suggest SAH
- Arterial puncture at non-compressible site in previous 7 days
- History of previous ICH
- Elevated BP (systolic >185 mmHg or diastolic >110 mmHg)
- Evidence of active bleeding on examination
- Acute bleeding diathesis, including but not limited to
- Platelet count <100,000/mm3
- Heparin received within 48 hours, resulting in aPTT >upper limit of normal
- Current use of anticoagulant with INR >1.7 or PT >15 seconds
- Blood glucose <50 mg/dl
- CT demonstrates multilobar infarction (hypodensity >1/3 cerebral hemisphere)
Only minor or rapidly improving stroke symptoms (clearing spontaneously) Seizure at onset with postictal residual neurologic impairments Major surgery or serious trauma within previous 14 days Recent GI or urinary tract hemorrhage (within previous 21 days) Recent AMI (within previous 3 months)
Inclusion Criteria
Diagnosis of ischemic stroke causing measurable neurologic deficit Onset of symptoms 3 to 4.5 hours before beginning treatment
Age >80 years Severe stroke (NIHSS >25) Taking an oral anticoagulant regardless of INR History of both DM and prior ischemic stroke
At present, use of IV rtPA within 3 to 4.5 hour has not yet been FDA approved, although it is recommended by current AHA/ASA science advisory
BP Management Glycemic Control: hyperglycemia should be treated with insulin when glucose >185 mg/dL Temperature Control: treat fever >37.5°C Dysphagia Screening Observe for signs of IICP: severe stroke, posterior circulation, stroke younger patient
Infuse 0.9 mg/kg (maximum dose 90 mg) over 60 minutes with 10% of the dose given as a bolus over 1 minute.

2010年10月20日 星期三
2010 CPR 與 ECC 準則提要
Highlights of the 2010 AHA Guidelines for CPR and ECC
2010 年 美國心臟協會 CPR 與 ECC 準則提要
高品質 CPR
- 胸部按壓速率:每分鐘至少 100 次 (快速壓)
- 胸部按壓深度:至少 5 公分 (用力壓)
嬰兒和兒童按壓深度至少為胸部前後徑的 1/3
(嬰兒約為 4 公分,兒童約為 5 公分)
- 每次按壓後確保完全的胸部回彈
- 儘量避免中斷胸部按壓
- 避免過度通氣
BLS的順序從 A-B-C 變更為 C-A-B單一施救者施行急救時建議之 30:2 按壓吹氣比並未變動
確認高級呼吸道裝置的位置後,可以繼續胸部按壓 (每分鐘至少 100 次) 且不需再配合通氣週期

- 立即確認心臟停止並啟動EMS
- 儘早 CPR
- 快速去顫
- Advanced Life Support
- 心臟停止後照護 (Post-Cardiac Arrest Care)


- 強調胸部按壓
- 單人施救者的在進行急救人工呼吸前開始胸部按壓 (C-A-B 而非 A-B-C)
- 單人施救者應以 30 次按壓開始 CPR,而非先進行 2 次通氣,以減少第一次按壓前的延遲
- 「看、聽和感覺是否有呼吸」已經從流程中移除
- 未經 CPR 訓練的一般民眾應實施 Hands- Only CPR (單純壓胸 CPR),直到取得 AED
- 經訓練的施救者如果能執行人工呼吸, 按壓吹氣的比率為 30:2
CPR 金字塔:CPR 期間使用團隊作業模式

電擊治療
- 任何施救者目擊到院前心臟停止,且現場可立即取得 AED,則施救者應以胸部按壓開始 CPR,並儘快使用 AED
- 建議實施單一電擊,接著立即進行 CPR ,而非連續3次電擊去顫
小兒去顫
- 初始能量:2 焦耳/公斤
- 後續能量:至少 4 焦耳/公斤,但不應超過 10 焦耳/公斤或成人最大劑量
- Af:初次雙相能量 120-200 焦耳;初次單相能量 200 焦耳
- AF:初次能量 50-100 焦耳 (單相或雙相)
- VT:初次能量 100 焦耳 (單相或雙相)
- 建議進行量化波形二氧化碳濃度監測 (quantitative waveform capnography),以確認並監控氣管內管位置與 CPR 品質
- 心臟停止後照護,改善入院心臟停止患者 ROSC 之後的存活率。治療包括心肺與神經系統方面的維持、低溫治療、PCI、診斷癲癇的EEG
- ROSC 後,FiO2 應調整到 SpaO2 ≧94% 所需的最小濃度

2010年10月19日 星期二
2010 Guidelines for CPR & ECC

2010 AHA Guidelines for CPR and ECC Science
- Executive Summary
- Evidence Evaluation and Management of Potential or Perceived Conflicts of Interest
- Ethics
- CPR Overview
- Adult BLS
- Electrical Therapies: AED, Defibrillation, Cardioversion, and Pacing
- CPR Techniques and Devices
- Adult ACLS
- Post–Cardiac Arrest Care
- Acute Coronary Syndromes
- Adult Stroke
- Cardiac Arrest in Special Situations
- Pediatric BLS
- PALS
- Neonatal Resuscitation
- Education, Implementation, and Teams
- First Aid
2010 International Consensus on CPR and ECC Science with Treatment Recommendations
兩個版本相較,10月19日的版本內容較多,但幾乎沒有圖表。根據AHA官網說明,11月2日的版本是10月19日版本的再版 (reprint),有較多的彩圖,內容也較簡潔,適合當醫院或醫療照護者的治療參考。個人建議下載11月2日的版本就好。
2010年10月16日 星期六
Consensus on GU Trauma
Consensus on GU Trauma
Evaluation and management of renal injuries:
consensus statement of the renal trauma subcommittee
BJU International Volume 93 Issue 7 Page 937-954, May 2004
INITIAL EVALUATION OF THE PATIENT WITH RENAL INJURY
URINE ANALYSIS
- The urine analysis is the most important laboratory study used to assess the patient with suspected renal injury.
- Hematuria is a common sign of renal trauma, being present in 80–94% of cases.
- There is no absolute relationship between the presence, absence or degree of hematuria and the severity of the renal injury.
- It is strongly recommended that patients with suspected penetrating kidney injuries have complete radiographic staging or renal exploration.
- Hemodynamically stable adults with blunt trauma should undergo radiographic evaluation if they have gross hematuria, microhematuria and SBP < 90 mmHg.
- Despite the absence of hematuria or shock, vertical deceleration injuries, in particular those associated with multiple-system injuries and/or physical signs of potential renal injury (flank ecchymosis, flank pain), demand renal imaging.
- Most children with microscopic hematuria do not require imaging.
- Hemodynamically stable children with blunt trauma should undergo radiographic evaluation if they have gross hematuria or > 50 RBCs/high-power field on microscopic urine analysis.
CT
- Abdominal CT with contrast medium is the best initial imaging study in patients with suspected renal injury.
- CT accurately identifies vascular injury, parenchyma laceration, urinary extravasation and perirenal haematoma.

INTRAOPERATIVE ONE-SHOT IVU
- When blunt or penetrating injuries cause massive hemorrhage and require immediate laparotomy, CT is contraindicated.
- Intra-operative one-shot IVU, in conjunction with findings at laparotomy, can be used to exclude life-threatening renal injury and confirm the existence of a contralateral functioning kidney.
- US is not invasive and has a high negative predictive value (96–98%), and therefore it is a good screening test for children and adults with presumed minor trauma.
- The reported accuracy of IVU in renal trauma varies from 65% to 95%, but the presence of abnormality on IVU usually requires CT or angiography to delineate the precise extent of injury.
- Its main usefulness may be to detect a normally functioning kidney on the uninjured side.
- Indications for angiography include suspected renal arterial thrombosis or segmental arterial injuries for which embolization or stenting is considered.
- In renal artery injuries, CT can be diagnostic and hasten operative intervention without angiography.
Absolute
- Persistent, life-threatening haemorrhage believed to stem from renal injury
- Renal pedicle avulsion (grade 5 injury)
- Expanding, pulsatile or uncontained retroperitoneal haematoma (thought to indicate renal pedicle avulsion)
- A large laceration of the renal pelvis, or avulsion of the PUJ
- Coexisting bowel or pancreatic injuries
- Persistent urinary leakage, postinjury urinoma or perinephric abscess with failed percutaneous or endoscopic management
- Abnormal intra-operative one-shot IVU
- Devitalized parenchymal segment with associated urine leak
- Complete renal artery thrombosis of both kidneys, or of a solitary kidney, or when renal perfusion appears to be preserved
- Renal vascular injuries after failed angiographic management
- Renovascular hypertension
OPERATIVE MANAGEMENT OF RENAL INJURIES
EARLY VASCULAR CONTROL
RENAL RECONSTRUCTION
NEPHRECTOMY
- The nephrectomy rate for immediate exploration of major renal lacerations in clinically unstable patients may reach 100%.
- Nephrectomy is still the most expeditious method of managing renal vascular injuries, and whereas renal artery repair is rarely possible and seldom successful.
- Successful selective renal artery embolization for managing hemorrhage in stable patients after blunt and penetrating renal trauma was reported by several centres.
- Primary angiographic management of renal vascular injuries has been advocated with surgical exploration reserved for those in whom it fails.


2010年10月13日 星期三
專科護理師執業範圍
專科護理師執業範圍 from Sun YaiCheng
扯 醫院竟讓護士縫傷口 辯「大家都這樣做」 院方已移送法辦
蘋果日報 2010年10月08日
護理師代醫師插管 病人猝死爆糾紛
自由時報 2007年1月9日
護理人員法 第四章 業務與責任
第 24條 護理人員之業務
- 健康問題之護理評估
- 預防保健之護理措施
- 護理指導及諮詢
- 醫療輔助行為
第 26條 病人危急時之處理方式
護理人員執行業務時,遇有病人危急,應立即聯絡醫師。但必要時,得先行給予緊急救護處理。NP執業範圍
- 住院病人身體理學檢查之初步評估及病情詢問。
- 紀錄住院病人病情及各項檢查、檢驗結果。
- 處理住院病人及其家屬醫學諮詢及病情說明。
- 在醫囑或醫師指示下,得開立檢驗、檢查申請單,但該檢驗、檢查申請單需註明醫師之姓名及時間,該指示醫師並應於24小時內,依醫師法及醫療法之相關規定,親自補開立檢驗、檢查單。
- 在醫囑或醫師指示下,得開立領藥單,但該領藥單上需註明指示醫師之姓名及時間,該指示醫師應於24小時內,依醫師法及醫療法之相關規定,親自補開立處方箋 。
- 其他經中央衛生主管機關認定宜由專科護理師執行之醫療輔助行為。
- 上述執業內容,應在醫院成立專科護理師執業委員會制定Clinical nursing guideline或Clinical nursing pathway後執行。
按醫療行為除診斷、處方、手術、病歷記載、施行麻醉等,應由醫師親自執行外,其他如注射、給藥、復健等治療行為,依醫師法第28條第1項但書第2款「在醫療機構於醫師指示下之護士、助產士或其他醫事人員」之規定意旨,得由護士、助產士或其他醫事人員在各該專業範圍下依照醫囑執行之,不限於醫師親自在場指示,…。
- 輔助施行侵入性檢查
- 輔助施行侵入性治療、處置
- 輔助各項手術
- 輔助分娩
- 輔助施行放射線檢查、治療
- 輔助施行化學治療
- 輔助施行氧氣療法(含吸入療法)、光線療法
- 輔助藥物之投與
- 輔助心理、行為相關治療
- 病人生命徵象之監測與評估
- 其他經中央衛生主管機關認定之醫療輔助行為
傷口縫合為高度專業技術,並具有相當之危險性,係屬手術連續過程之一環,應由醫師親自為之。
專科護理師如執行前揭業務,業已逾越其專業人員法律之規定放置鼻胃管相關函釋
將外來物之鼻胃管經由病患鼻腔、咽喉、避開大氣管、深入食道到達患者胃部,以為引流、抽吸或灌食、給藥之行為,屬侵入性治療及處置
因鼻胃管初次置入仍有相當程度之危險性,宜由醫師親自為之
至鼻胃管全管拔除及需長期鼻胃管留置患者之定期更換,如經醫師診察、判斷後,得可指示護理人員協助之
2010年10月8日 星期五
Acetylcysteine for Acetaminophen Poisoning
Acetaminophen Poisoning
View more presentations or Upload your own.
Acetylcysteine for Acetaminophen Poisoning
N Engl J Med. July 17, 2008;359:285-92
4 Stages of Acetaminophen Poisoning
- Preclinical toxic effects (normal ALT)
- Hepatic injury (elevated ALT)
- Hepatic failure (hepatic injury with hepatic encephalopathy)
- Recovery
Clinical Use
It is prudent to administer acetylcysteine to any patient with an elevated ALT and a history of ingesting more than 4 g of acetaminophen per day.
The Rumack–Matthew Nomogram

Dosing of N-Acetylcysteine
FDA-approved protocols for treatment of acute acetaminophen ingestion:
- Oral acetylcysteine is loading dose 140 mg/kg, with maintenance doses 70 mg/kg Q4H for 17 doses.
- IV loading dose is 150 mg/kg over 15 to 60 minutes, followed by infusion 50 mg/kg over 4 hours, and finally infusion 100 mg/kg over 16 hours.
Many toxicologists would recommend repeating the measurements of ALT and acetaminophen concentrations as the patient approaches the end of the 16-hour infusion period and continuing treatment if the ALT is elevated or if the acetaminophen concentration is measurable.
OPD therapy may be considered for patients with a
- confirmed accidental
- repeated supra-therapeutic ingestion
- supra-therapeutic acetaminophen concentration (threshold of <70 µg /ml)
- low-grade elevation of the ALT (<3 times the upper limit of the reference)
The patient can be discharged with 3 maintenance doses to be taken every 4 hours and be re-evaluated 12 hours after the loading dose.
Treatment can be discontinued if the patient meets the criteria for stopping therapy (i.e., the ALT is decreasing, and acetaminophen concentration is undetectable).
Patients receiving intravenous acetylcysteine for liver failure should be hospitalized in ICU. Treatment is continued until the hepatic encephalopathy resolves and the ALT and creatinine and INR have substantially improved or until the patient receives a liver transplant.
Side Effects of N-acetylcysteine
- Vomiting is common with oral administration.
- The most commonly reported adverse effects of intravenous N-acetylcysteine are anaphylactoid reactions (15%), including rash, pruritus, angioedema, bronchospasm, tachycardia, and hypotension.
United Kingdom National Health Service guideline recommends treating patients who have acute acetaminophen overdose and a acetaminophen concentration above the probable-toxicity line (the line that begins at 200 µg/ml at 4 hours after ingestion) and high-risk (alcoholic or malnourished) patients who have a concentration above high-risk line that begins at 100 µg/ml at 4 hours.
American College of Emergency Physicians recommends acetylcysteine therapy for any patient with acute acetaminophen ingestion and a timed serum concentration above the line that begins at 150 µg/ml at 4 hours, as well as for any patient with liver injury or liver failure.
2010年10月5日 星期二
加拿大急診檢傷系統 簡介
自民國99年起,台灣急診全面實施急診五級檢傷分類標準。 台灣急診檢傷分類系統的主要參考架構是以加拿大五級檢傷與急迫量表(CTAS)為基礎,使用其系統之架構與內容,發展出台灣五級檢傷與急迫度量表(Taiwan Triage and Acuity Scale, TTAS)。 加拿大檢傷與急迫度量表(Canadian Triage and Acuity Scale, CTAS)  CTAS 依急診病患嚴重度分級之候診時間的標準
CTAS 依急診病患嚴重度分級之候診時間的標準
CTAS 依急診病患嚴重度分級之候診時間的標準
1級為危及生命需立刻急救者 Resuscitation → 應立即處理
2級為危及生命需緊急處置者 Emergency → 應在15 分鐘內處理
3級為可能危及生命屬緊急者 Urgent → 應在30 分鐘內處理
4級為生命穩定屬低度緊急者 Less-urgent → 應在60 分鐘內處理
5級則無危及生命屬非緊急者 Non-urgent → 應在120 分鐘內處理並強調病患在急診候診區等待看診時,護理人員必須做再次評估 re-assessment,以確保病患病情變化,若與初步評估不同,可更改急診檢傷級數。 評估急診檢傷級數遵循條件 Assignment of Triage Level
- 目前主訴 (presenting complaint):先產生最低限度級數(主訴仍是決定分級的主要因素)
- 第一次修正級數:可根據生命徵象 (vital signs)、血流動力、意識、呼吸窘迫與體溫等程度不同而變更級數
- 疼痛嚴重度 (pain severity):分為中樞型/周邊型或急性/慢性疼痛。分級以變數中最嚴重的項目作為基準,如:病患有正常的生命徵象,依據目前主訴可能判定為3、4或5級,但若有嚴重中樞型疼痛則依據疼痛量表修改為2級
- 外傷機轉 (mechanism of injury):外傷病患高危險性機轉,如:高速車禍(時速 > 60 公里)、車禍時車輛翻滾、乘客被拋出車外或同車乘客死亡,車輛空間被擠壓、救援時間 > 20 分鐘、行人/腳踏車被撞或輾過、6公尺以上跌落等,判定檢傷2級
- 第二次修正級數,針對無法由第一次資料修正加以界定時的特殊主訴,可進行檢傷級數修正,如:化學傷害部位為眼睛則判定為2級
ppt 部分格式與動畫在 slideboom 上播放會有失真的現象,如要觀看精彩完整動畫效果,請下載 原始檔案,並使用 powerpoint 2007 or 2010 播放相關文章: 台灣急診五級檢傷系統 美國急診檢傷系統 簡介
2010年10月1日 星期五
Post-Cardiac Arrest Syndrome
Post-Cardiac Arrest SyndromeEpidemiology, Pathophysiology, Treatment, and Prognostication A Consensus Statement From the International Liaison Committee on Resuscitation Circulation. 2008;118:2452-2483 Background
- CPR→ ROSC→ Resuscitation→ Post-CardiacArrest Syndrome (PCAS)
- The largest published in-hospital cardiac arrest database (the NRCPR) includes data from > 36000 cardiac arrests.
- In-hospital mortality rate was 67% for the 19,819 adults with any documented ROSC, 62% for the 17,183 adults with ROSC > 20 minutes.
- Post-Cardiac Arrest Brain Injury
- Post–Cardiac Arrest Myocardial Dysfunction
- Systemic Ischemia/Reperfusion Response
- Persistent Precipitating Pathology
- Monitoring
- Early Hemodynamic Optimization
- Ventilation
- Circulatory Support
- Management of ACS
- Therapeutic Hypothermia
- Sedation and Neuromuscular Blockade
- Seizure Control and Prevention
- Glucose Control
- Placement of Implantable Cardioverter-Defibrillators

- Patients resuscitated from cardiac arrest who have ST-elevation myocardial infarction should undergo immediate coronary angiography, with subsequent PCI if indicated.
- It is appropriate to consider immediate coronary angiography in all post-cardiac arrest patients in whom ACS is suspected.
- Unconscious adult patients with ROSC after out-of-hospital VF cardiac arrest should be cooled to 32°C to 34°C for at least 12 to 24 hours.
- Rapid IV infusion of ice-cold 0.9% saline or Ringer’s lactate (30 mL/kg) is a simple, effective method for initiating cooling.
- Slow rewarming: 0.25°C to 0.5°C per hour.
- If therapeutic hypothermia is not undertaken, pyrexia during the first 72 hours after cardiac arrest should be treated aggressively with antipyretics or active cooling.
- Prolonged seizures may cause cerebral injury and should be treated promptly and effectively with benzodiazepines, phenytoin, valproate, propofol, or a barbiturate.
- Clonazepam is the drug of choice for the treatment of myoclonus.
- Tight control blood glucose (80 to 110mg/dL) with insulin.
- In survivors with good neurological recovery, insertion of an ICD is indicated if subsequent cardiac arrests cannot be reliably prevented by other treatments (such as pacemaker for AV block, transcatheter ablation of a single ectopic pathway, or valve replacement for critical aortic stenosis).
訂閱:
文章 (Atom)








{kind=link}